Project background
In recent years, recovery-based approaches have reshaped thinking about mental health care across the UK. Rather than focusing primarily on a rehabilitative or medical model led by professionals, recovery approaches place greater emphasis on the person experiencing mental distress, their hopes, strengths, choices, and ability to live a meaningful life.
The recovery model is often understood as a way of living a satisfying, hopeful, and contributing life, even when a person continues to experience the effects of mental health difficulties. In this context, person-centred care has become central to how support is designed and delivered. It encourages services to look beyond symptoms and treatment and to recognise people as experts in their own lives.
However, applying recovery-based approaches in practice is not always straightforward. Some people argue that the model can oversimplify the complex social, emotional, and structural factors connected to mental distress. There is also no single shared definition of recovery, which can make it difficult to evaluate how well the approach is being used or understood across different services and settings.
The IMPACT Network, running from November 2024 to April 2025, was developed to explore recovery-based approaches as an important issue for improving the lives of people experiencing mental distress, as well as their carers. It brought together a range of perspectives to consider how recovery principles can be meaningfully embedded in mental health support.
The Network provided a space to examine the value of recovery-based approaches, the challenges involved in applying them, and the conditions needed for them to work well in practice. By connecting people with different experiences and expertise, the project aimed to support more responsive, inclusive, and person-centred mental health care. Ultimately, this work is about identifying practical solutions for implementing the recovery model in ways that reflect people’s own personal meanings of recovery, ensuring support is shaped by their priorities, values, hopes, and lived experiences.
IMPACT Factfile
- Year: 2024 – 2025
- Delivery Model: Networks
- Themes:
- Resources:
Network members
Networks were co-ordinated by:
Networks in England
Is a growing mental health charity in the South East of England committed to supporting our local residents in Dartford, Gravesham, Swanley and Medway.

Is on a mission to bring about meaningful change to our health and social care system, to the way society views mental illness, and to people’s lives across the country.

A small Community interest company founded in 2010. Community Glue works with other groups, organisations and individuals to help people who use health and social care services get better support.

Networks In Scotland
Networks In Northern Ireland
Has been walking alongside people across Scotland who are experiencing mental health challenges for more than 40 years.
is a Senior Strategic Improvement Coach at IMPACT (Improving Adult Social Care Together). She coordinated a network in Northern Ireland.

Evidence review
Each Network starts with an evidence review conducted by the IMPACT team.
Although there is no univocal definition of recovery, there is consensus that recovery does not necessarily imply only the “cure“. However, evidence noted that health professionals, and often people using mental health services, are not aware of the distinction between ‘recovering’ (the process) and ‘recovery/recovered’ (the outcome). There are two main meanings of the term “recovery” in mental health systems internationally:
1. The biomedical or traditional model aims for clinical (or scientific) recovery. In other words, it seeks recovery from mental illness.
2. The recovery-based approach to mental health aims for personal or social recovery, meaning recovery from a mental illness.
The recovery-based approach stemmed from various civil rights movements, starting in the 1960s, as a response to stigma and suppression in the psychiatric system. These movements are based on
ideas of human rights and empowerment. The term “recovery”, as it is used by the recovery-based approach, first appeared in the 1980s through the consumer/survivor movement.
The central idea of the recovery revolution was that mental illness is only one element in a person’s life. For this reason, recovery cannot be reduced to the “cure” of symptoms. It must encompass the illness while pursuing a full and meaningful life despite its challenges.
Recovery models help to challenge negative attitudes and assumptions that people living with severe mental health conditions can only get worse.
The evidence review highlighted that a recovery-based approach has positive implications both for people using services and practitioners (Martinelli and Ruggeri, 2020).
● Better outcomes for people with mental distress;
● Reduction of health costs;
● Greater value on the personal knowledge of the individual and balance in the power which historically was held by psychiatrists and professionals in the mental health care service;
● A better focus on the personal priorities of the person using the services rather than on what is defined by the professionals.
Evidence also highlighted the main barriers to the implementation of recovery-based approaches: In the UK, the dominant approach applied in the mental health system is the biomedical model. There is a general lack of clear definitions of what a ‘recovery-based practice’ is – this means that it It is very difficult for organisations and professionals to put this model into practice. The recovery model emphasises the process rather than the outcome – this makes it very difficult to assess the effectiveness of this approach.
The evidence review highlighted that a recovery-based approach has positive implications both for people using services and practitioners (Martinelli and Ruggeri, 2020).
● Better outcomes for people with mental distress;
● Reduction of health costs;
● Greater value on the personal knowledge of the individual and balance in the power which historically was held by psychiatrists and professionals in the mental health care service;
● A better focus on the personal priorities of the person using the services rather than on what is defined by the professionals.
Evidence also highlighted the main barriers to the implementation of recovery-based approaches:
In the UK, the dominant approach applied in the mental health system is the biomedical model. There is a general lack of clear definitions of what a ‘recovery-based practice’ is – this means that it is very difficult for organisations and professionals to put this model into practice. The recovery model emphasises the process rather than the outcome – this makes it very difficult to assess the effectiveness of this approach.
The CHIME framework
The evidence review also highlighted one specific model – The CHIME framework describes five key processes that support personal recovery in mental health:
- Connectedness: building positive relationships with peers, communities and professionals.
- Hope: believing that recovery and a better life are possible.
- Identity: developing a positive sense of self beyond diagnosis or stigma.
- Meaning: finding purpose, value and belonging in everyday life.
- Empowerment: having choice, autonomy and confidence to shape one’s own recovery. (Leamy et al. 2011)
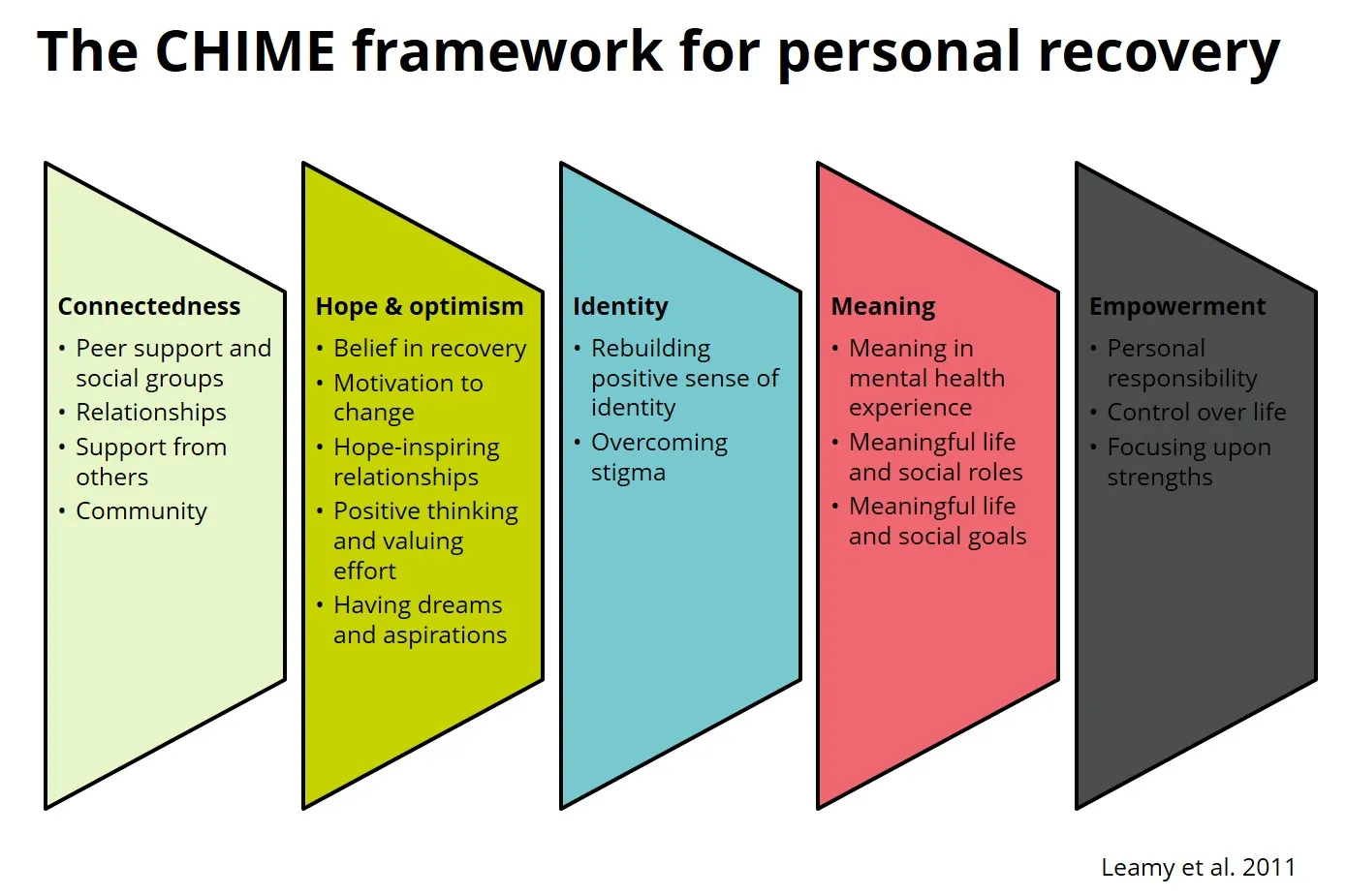
Diagram titled “The CHIME framework for personal recovery” showing five coloured panels: Connectedness, Hope and optimism, Identity, Meaning, and Empowerment. Source: Leamy M, Bird V, Le Boutillier C, Williams J, Slade M. Conceptual framework for personal recovery in mental health: systematic review and narrative synthesis. Br J Psychiatry. 2011 Dec;199(6):445-52. doi: 10.1192/bjp.bp.110.083733. PMID: 22130746.
Policy Context Across the UK
The evidence also highlighted that recovery-based approaches are now embedded in mental health policy across the 4 UK nations, but the emphasis and implementation vary.
● Scotland led the way, with recovery made a central policy priority after devolution and supported through the Scottish Recovery Network.
● England has strongly promoted recovery in national mental health policy, though implementation is often constrained by medical-model practice and professional-led approaches.
● Wales has built recovery principles into service restructuring through the Mental Health Measure, particularly around self-management, co-production and care planning.
● In Northern Ireland, recovery has gained ground following the Bamford Review and Recovery Colleges, but progress is still limited by funding pressures and continued dominance of the medical model.
The Networks explored the existing evidence on Recovery-Based approaches on the basis of their experiences of recovery from their lived experience and professional knowledge. When discussing the existing evidence on recovery-based approaches, Network members said:
- The contrast between recovery-based and medical approaches is too simplistic. Recovery in mental health should not be reduced to a binary choice. Instead, the two models can work together.
- Recovery holds different meanings, and these meanings can change for the same person throughout their life. “Everyone is different; there is no ‘set in stone’ way to deal with people, as we have our own journeys.”
- Recovery is closely connected to community life. Therefore, raising awareness and educating people about mental illness should be part of recovery support.
- Evidence tends to focus heavily on the medical aspects of mental illness. However, everyone could experience mental health challenges at some point, which may not require medical attention but rather community support.
When looking at what works, Networks recognised the CHIME Framework as a good framework because of the following reasons:
“Empowerment really stands out to me.”
“It emphasises the importance of the social Network”
“I can relate to the part about meaning – I care about the meaning I find in my life and what I’m involved in.”
The following models were identified as good practices:
- Peer support
- Supported housing
- Volunteering and employment as activities to improve self-worth, give motivation, and empower the person
- Choices of treatment and better information to access support and services were identified as key to avoid crises.
- A strength-based approach to support recovery – identifying what is already existing in the community as a strength to support recovery.
- Being involved in the community and being an active citizen – Having their own voices heard in commissioning and in planning their own care is an important empowering factor, and it would allow more person-centred services.
- Good co-production or more radical approaches, such as developing their own user-led services, could lead to power-sharing initiatives.
- When looking into the implementation of recovery-based approaches, network members highlighted some systemic challenges:
- Limited resources and funding compromise the proper implementation of recovery models. A key question is how to sustain mental health recovery with short-term projects and interventions.
- Some challenges are linked to applying the model according to diagnosis. For example, when people lack awareness of their condition’s severity or are in an acute state of addiction, the recovery model may not fit. Participants also noted that recovery is not tied to diagnosis. One network compared it to diabetes: “You don’t recover from diabetes, but you can live well with it.”
- Stigma and language continue to create barriers to accessing recovery-based services. People remain afraid of being labelled as having a mental illness. Therefore, members suggested using the term “well-being”, which feels more acceptable.
- Community services and peer support often lack sufficient funding.
- Co-production must go beyond consultation. If services are led solely by statutory bodies and professionals, power imbalances remain, undermining the empowering purpose of co-production.
- Involvement of people with lived experience in Integrated Care Board (ICB) commissioning remains too limited. When statutory services dominate decision-making, power imbalances are particularly strong.
In meetings 3 and 4, Networks developed their action plans using the theory of change; these are only a few snapshots of the changes they wanted to see and potential actions.
Laura Doyle’s Network
This Network identified two main areas for action, which are linked:
● Individuals who were keen to share their recovery stories and experiences
● Those interested in discharge planning and the provision of information
They decided to co-produce a video – collecting positive stories of recovery to be shared as peer support for other people. You can learn more about the process.
Laura Doyle interviewing network members during the shooting of the video.

Rethink Network
This Network was focused on recovery-based approaches to mental health in secured settings. Their action plan focused on the application of Recovery-based approaches in secured settings:
- Including people with lived experience in planning their recovery plan;
- Improving communication with community services.
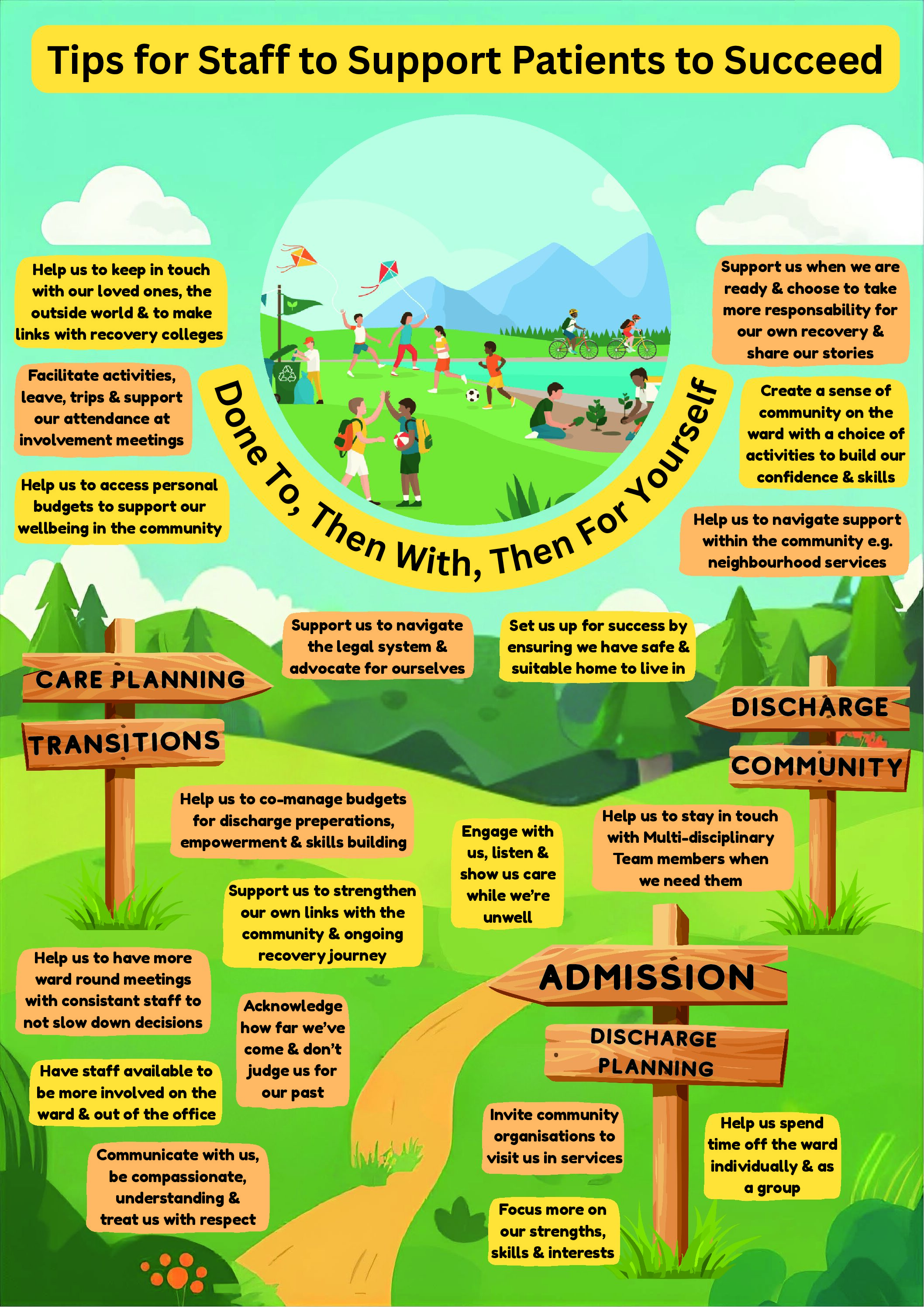
The Network coproduced a ‘top tips resource’ for professionals from the point of view of Experts by Experiences, which was also translated into an easy-read version.
Rethink Network coproduced poster: Top tips to support patients to succeed
Rethink Network Top Tips poster: A colourful illustrated poster titled “Tips for staff to support patients to succeed”. It shows a recovery journey through secure care, with a winding path and signposts for Admission, Care Planning,Transitions, Discharge Planning, Discharge, and Community. Around the scene are patient-led tips asking staff to communicate with compassion and respect, focus on people’s strengths, support independence, involve loved ones and community links, and help with planning for discharge and ongoing recovery. Learn about the process creating the top tips poster
Top tip resource easy-read version
Community Glue Network
This Network, which is coordinated by a Community Interest Company in Oxford, looked into the importance of the community in the process of recovery. “It’s useful for people to be able to think through the issues they face without always having to focus on symptoms and diagnosis.” As part of their action plan, they set up a local recovery Network and co-designed a credit-card-sized resource for community groups and organisations that are not mental health specialists but are supporting people recovering from mental distress. This would incorporate the CHIME framework and details of local organisations and groups.
Community Glue leaflet: “What helps our mental wellbeing?”
The Community Glue leaflet explains the five CHIME recovery factors: Connection, Hope, Identity, Meaning and Empowerment. Each section gives short, practical examples, such as building positive relationships, believing recovery is possible, developing a positive sense of self, finding meaning through work, community, nature or hobbies, and taking more control over everyday life. The leaflet uses simple illustrations, including wind chimes, a candle, people having tea, and a raised hand holding tools.
{kind=link}
