Award Success at 2024 Social Policy Association Awards

We are thrilled to share some good news from this …
We are thrilled to share some good news from this …

The latest IMPACT academic seminar brought together leading practitioners and …

Emily Holzhausen, our Leadership Team thematic lead for carers and …
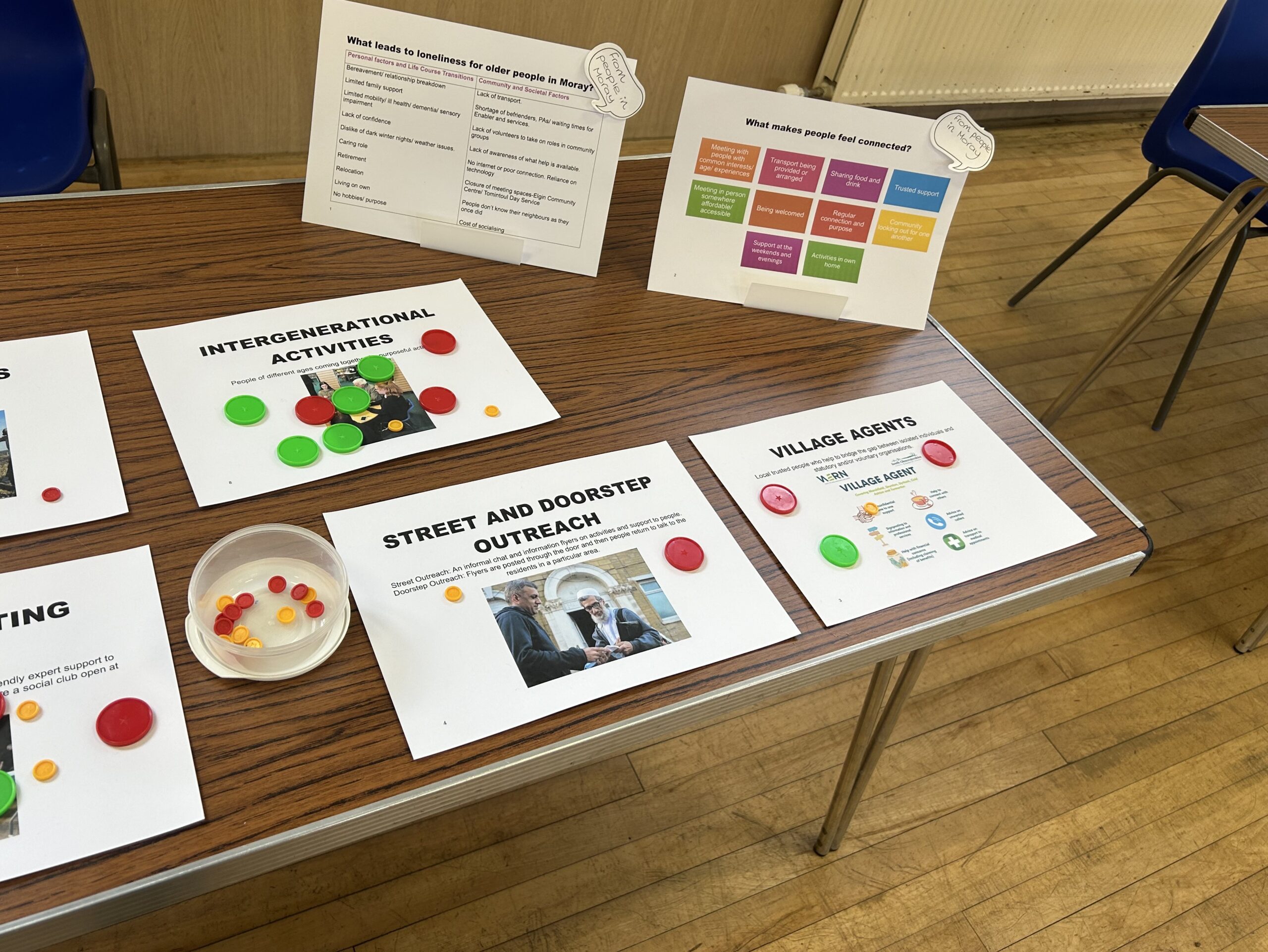
In March, InKeith and Strathisla and partner, LEAD Scotland (Linking …
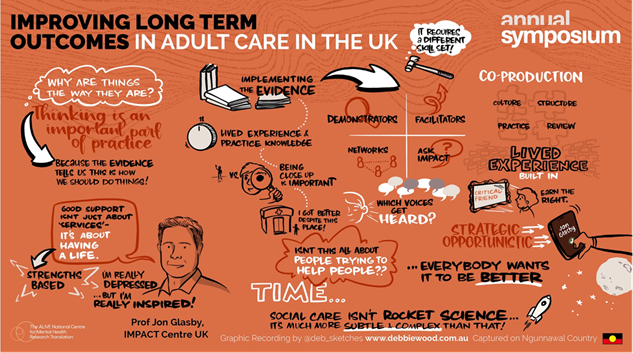
Jon Glasby, IMPACT’s Director, has been in Australia representing IMPACT …
IMPACT (Improving Adult Care Together), the UK centre for implementing …

Collaboration for the best outcomes within adult social care is …