As part of the IMPACT Network on recovery-based approaches to mental health, Paulina Navarro from Rethink Mental Illness, on behalf of her wider team, reflects on the importance of embedding lived experience, collaboration and person-centred practice within secure mental health care settings.
The IMPACT Recovery-based Approaches to Mental Health Network, led by Rethink Mental Illness, brought together a variety of perspectives. Together we explored what recovery really means in secure care settings – and how services can better support it.
This focus was in response to recovery often being unintentionally misunderstood, constrained by risk-based systems or treated as a linear journey within secure care contexts. Across our sessions, members challenged this and worked together to co-produce practical, experience-led resources to influence policy, practice and culture.
Our approach
The Network brought together a diverse group of Experts by Experience (EbEs) from medium- and low-secure services; staff members who supported patient involvement as well as contributed their own professional perspectives; and a researcher specialising in recovery who had previously been a consultant psychiatrist.
Creating a space where these perspectives could sit alongside one another was central to the Network’s approach. Sessions were facilitated by Rethink’s Lived Experience Insights team to prioritise safety, accessibility and meaningful contribution. This supported members to speak openly about their thoughts on the current research and evidence around recovery and what had – and hadn’t – supported their own recovery journeys.
Key themes from the Network
Across our sessions and discussions, consistent themes emerged:
- Recovery is not linear but deeply personal, iterative and self-defined
- Members felt that research, policy and practice too often present recovery as a straightforward path with predictable stages or outcomes. In reality, people described recovery as something that includes setbacks, pauses, changes in direction and periods of uncertainty. Framing recovery as linear was felt to be not only inaccurate but also harmful – particularly in secure care, where progress is often tied to risk assessments and rigid pathways.
- Decisions are too often made about people, not with them
- Many members shared frustration about key decisions – such as care plans, leave, risk assessments and discharge planning – being made for them rather than with them. This lack of involvement left people feeling disempowered and disconnected from their own recovery. Members highlighted how these dynamics can undermine trust and contribute to people becoming “stuck” in secure services longer than necessary.
- Relationships, trust and time matter
- Trusting relationships between staff and patients were repeatedly identified as key to recovery. Members spoke about the impact of frequent staff changes, limited time for meaningful conversations, infrequent ward rounds and slow decision-making. Without time and continuity, trust cannot develop – and without trust, people struggle to feel safe enough to take responsibility for their own wellbeing or plan for life beyond secure care.
- Collaboration supports progress
- The Network highlighted the importance of staff and patients working collaboratively. Recovery was seen as something that should happen with people, not something that is delivered to them. Peer support, co-production, recovery colleges, meaningful activity and community engagement were all identified as practical ways to support this collaborative approach – particularly when preparing for transitions out of secure care and into the community
From discussion to action: co-producing a practical tool
As the Network moved into its action-planning phase, members were clear that they wanted to produce something practical, accessible and grounded in lived experience. Through a theory of change approach, we planned a resource that could capture the learning and discussion from the Network and encourage staff working in secure care to work more collaboratively with patients using practical tips. We wanted the output to reflect the recovery journey as non-linear and offer realistic, experience-based guidance
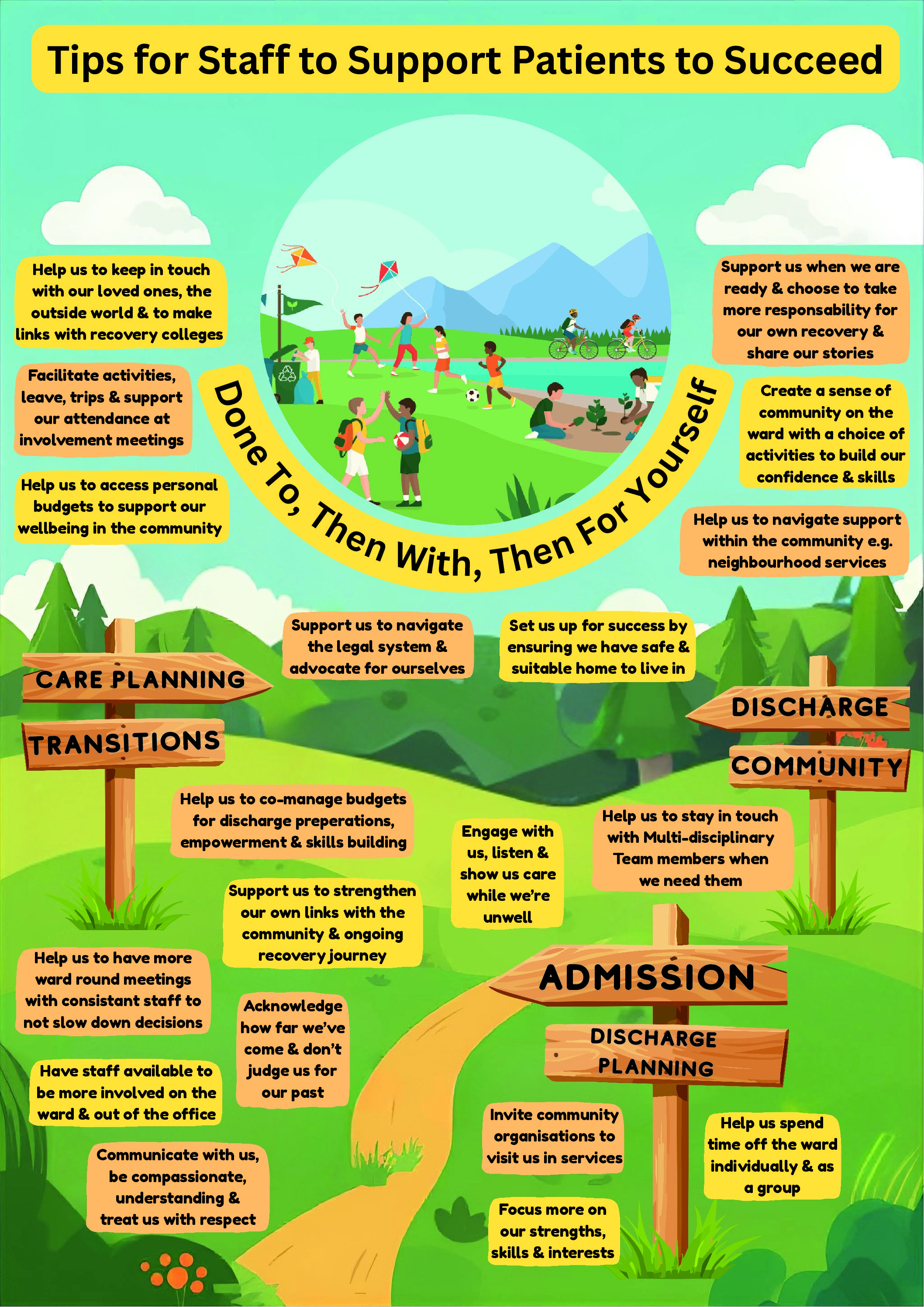
The ‘top tips for recovery’ poster
Over several co-production sessions following the Network’s initial four meetings, members worked together to create a poster outlining the recovery pathway and sharing tips to support this journey. The imagery presents recovery as a non-linear pathway, showing signs that indicate a direction moving forward but allowing for pauses and setbacks. These signposts are surrounded by practical tips for staff, linked to the different stages of recovery.
These tips highlighted key areas from members’ experiences, such as more meaningful time between patients and staff for building trust and developing relationships. Also supporting access to meaningful activities such as hobbies, volunteering and work with choice and flexibility. Transitions were also a key element, such as ensuring access to safe and suitable housing and supporting reintegration into the community and setting people up to succeed long-term.
The title of the poster came directly from a Network member, who described recovery as a shift from care being “Done to, then with, then for yourself”. This phrase captured the Network’s shared belief that recovery in secure care should involve gradually transferring power and responsibility back to the individual person at a pace that feels safe and supported.
Feedback & learning
Once the poster was developed, it was shared with a wider group of stakeholders to gather feedback. At an in-person event, printed copies of the poster were shared with post-it notes to capture reflections and feedback from fellow patients, peer support workers, and patient engagement and support staff.
The response was overwhelmingly positive. People told us the pathway, imagery and tips resonated with their own experiences. At the same time, some raised concerns about accessibility, particularly for people with neurodivergence or those who may find dense visual information difficult to engage with. In response to this feedback, we worked with the Patient Experience and Involvement Lead for Learning Disabilities at a service in Oxford to co-develop an easy-read version of the poster. We are happy to have both available to download from IMPACT’s website, so there is the option of two formats.
What’s next
The learning from this Network continues to inform Rethink Mental Illness’s influencing and engagement work within secure care services and provider collaboratives. We will be launching a new IMPACT Network later this year on developing ‘neighbourhood health’ approaches/integrated neighbourhood teams and carrying forward many of the key messages and themes around this work on how patient experiences and recovery can be better supported, more holistic and person-centred.