6-week reflection by Amber Cagney, Networks Manager
I’m Amber Cagney – I work part-time with Kate Hamblin (Networks Lead) and Maria Teresa Ferazzoli (Project Officer) on the IMPACT Networks. My role is UK Networks Manager, which includes recruiting Local Network Coordinators across the four nations, supporting them to run their Local Networks and meeting them in between each one to debrief and decide together how to run their next meeting. We’re currently running our first pilot network on choice and control and recruiting sites for the second network pilot on values-based recruitment and retention.
I worked in the anti-slavery sector for almost 10 years after starting out as a volunteer! My previous job with West Midlands Anti-Slavery Network was as the development manager where I set up a safe house project for male survivors of modern slavery in a multi-agency partnership. I still work within the sector part-time, and I’m a trustee for a charity delivering long-term support to survivors of modern slavery and human trafficking.
I’ve been with IMPACT for six weeks and am reflecting on the work we’ve done so far.
Equality, Diversity, and Inclusion
Equality, diversity, and inclusion are at the centre of IMPACT’s values. Having come from a human rights background, I believe the Universal Declaration of Human Rights should be central to any work or research into the care and support of people. The Declaration states “All human beings are born free and equal in dignity and rights”, it also states the rights to equal access to public services, the freedom of movement, and many others; these are core principles and it’s essential that our work is grounded in the pursuit of equality for all people to have a good life and the ability to thrive.
Equality is about ensuring that every individual has an equal opportunity to make the most of their lives and talents. It is also the belief that no one should have poorer life chances because of the way they were born, where they come from, what they believe, or whether they have a disability. Equality recognises that historically certain groups of people with protected characteristics, such as race, disability, sex, and sexual orientation, have experienced discrimination.
Multi-agency Interactions
IMPACT’s Networks are a good example of inclusive multi-agency interactions that are exploring the issues related to choice and control and values-based recruitment with a range of individuals who either draw upon care and support or help deliver it. Our first pilot is underway, tasked with exploring mechanisms, systems, and behaviours in adult social care that enable choice and control.
Initial Feedback
The feedback from our first Local Network meetings across England, Scotland, and Wales has been really interesting to read and reflect on so far. The definition of care is “the process of protecting someone and providing what that person needs”. The feedback strongly suggests the shift needs to be in the “process” and ensuring that the person being cared for has a voice, choice, and control in what their care looks like, with the recognition that every person is unique and has their own wants and needs. All individuals who access public services for care have the right to be protected from harm, and the right to be supported to live with as much autonomy and freedom as possible.
Choice and Control in Care
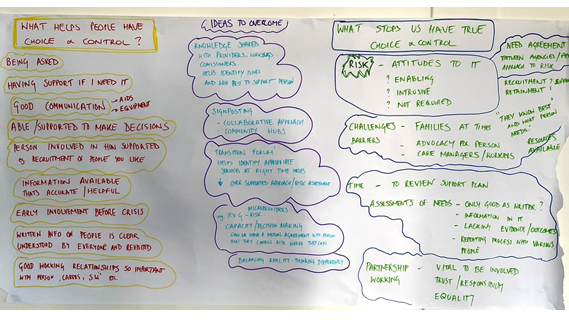
The networks discussed enablers for choice and control in care, which included:
- Being asked – sometimes decisions can be made for people. True choice and control means asking, then asking again in the future – not assuming one answer stands forever – and also considering the person’s communication needs.
- Being supported to make decisions – decision making can happen at lots of different levels, and people should be supported to make as many decisions as they can, and at every level possible.
- Good information – being able to access information on providers, activities, or groups, that is up to date and free from jargon, but also accessible.
- Good relationships – there are power dynamics in relationships, about how one person could be seen as being quite influential and pushing a decision in a particular way. Facilitating open conversations is important, potentially using advocacy.
- Transparent systems and clarity over budgets– clear understanding of the eligibility criteria for different monies and knowing what they could be spent on
The local network attendees also acknowledged hindrances and barriers to choice and control, including both systemic and human decisions such as:
- Risk – people should be supported to take risks and try new things, but attitudes – from the person, their family, support provider, or social worker – can be a hindrance. Proactive risk management with the supported person and mitigating risks together can be positive.
- Relationships – sometimes the “family knows best” perspective can be a hindrance to the individual making progress. Also relationships between different partners- care providers feel like they are consulted to a lesser degree than a social worker, for example.
- Rigid systems and processes
- Time – time to review support plans is not seen as a priority, and choices should be revisited, not taken as permanent.
- Location and availability of services – very rural locations mean choices can be limited.
- Disconnect between social care and health – health paying directly for some services rather than putting it into the budget so the individual can choose.
- Covid-19 – many projects and activities were paused during the COVID-19 pandemic.
Next Steps
The next steps of the Local Networks are to explore what an effective mechanism to enable choice and control with finances and support plans looks like, and to share best practice amongst the different regions
We are currently facing the ongoing challenges of the COVID-19 pandemic, in a complex adult social care environment that is systemically underfunded, undervalued, and neglected in policy; we are very aware of the challenges of creating change, however, to progress and move forward to a more equal society and nation, these are exactly the types of conversations we urgently need to have, and there is no better time than now.